
{kind=link}
It’s a Friday night, and you and your partner are watching the newest rom-com on Hallmark Channel getting ready for Christmas… all of a sudden, it’s time for a commercial, and two bathtubs appear out in the open with a couple now walking up to them. The commercials cuts, and we now watch the man and woman in the tub holding hands. The commercial ends with the always hilarious “If you have an erection that lasts longer than four hours, seek medical help immediately.” You just watched the smash hit Cialis commercial. Who can forget about the fun “Oh, Oh, Oh, OZEMPIC, you know” commercial either? I have sung that jingle to my first-year pharmacy students for a couple of years now. Last but not least, my new personal favorite is the “I take once daily Jardiance” jingle.
Advertisement
While these commercials often provide fun songs to sing along to, a more ominous voice comes over and lists all major side effects affiliated with the drugs, with the final one being “possible death.” Likely? Probably not, but the fact it needs to be mentioned is still comical. So, is this ok? Should Big Pharma be able to promote direct-to-consumer advertising? You’ll be shocked to learn that the United States and New Zealand are the only two countries in the world that allow for direct-to-consumer marketing of pharmaceutical products. Big Pharma will spend $30 billion on advertising this year, up 5 percent from last year.
Is this ethical? Probably not. Let’s dive in, shall we? Let’s use Jardiance, for example. Jardiance is a type 2 diabetes drug that works by blocking the sodium-glucose cotransporter 2, aka it stops sugar from being reabsorbed in the kidneys and forces the body to urinate it out. It does have a benefit in people at high risk of cardiovascular death, which makes it popular in the treatment of diabetes. Thirty pills cost (at wholesale price) about $585.00. The problem? In studies, it lowers A1c only about 0.7-0.9 percent. Goal A1c (the measure of blood sugar over three months) is <7 percent. Let's look at a popular drug that's been around much, much longer — metformin. Metformin, the generic for Glucophage, went generic in 2000. it costs actual pennies, and you can get a 90-day supply for about $5-10 at some pharmacies. It can lower A1c ~1.5-2 percent. It is pretty well tolerated, aside from some possible GI side effects.
Advertisement
Let’s say we have a diabetes patient with an A1c of 9 percent. That means your average blood sugar level is 212mg/dl. Reference for normal while fasting is 70-100 mg/dl, and a normal random draw should be less than 125mg/dl. Goal A1c is <7 percent. Which drug will get you there?
Which drug would you prefer? Personally, I’d want the cheaper, more effective metformin. However, when doctors get visited by pharm reps, or patients come in singing the jingle and put pressure on the doctors to write for the drug they like, we often see the less effective, more expensive drug written. Some may require prior authorization, which can hold up the process of getting medications to the patient. We can also see higher co-payments and less access to drugs for some patients. Does this mean we can’t add on Jardiance down the line if metformin doesn’t work? Of course, we can, as we can with the GLP drugs. Point being: If doctors are influenced by the pharm reps, the commercials, the patients, we end up costing the medical system much more than we need to when there are other drugs that can treat that disease more efficiently and for far less.
Who Do Pharmacy Benefit Managers Actually Benefit?
WATCH: Do You Live in a Pharmacy Desert?
So, why is this allowed? Well, it’s no shock that Big Pharma has a hand in getting our leaders elected. Looking at this chart…
Advertisement
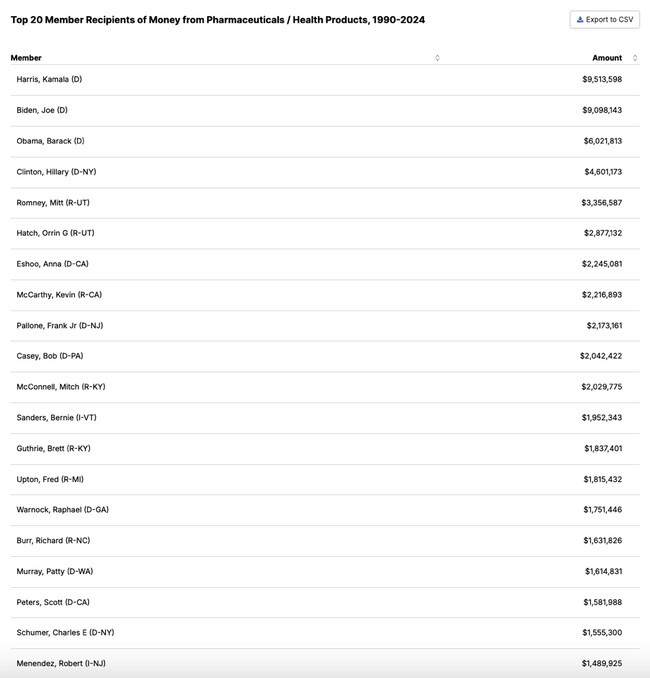
…they have a hand in who gets elected, and, one would assume, if Big Pharma helps get you elected, you won’t want to regulate the hand that feeds you. As with stock trading in Congress, which I will leave to others to dissect, Big Pharma should not have a hand in who we elect as leaders. This conglomerate should be more regulated and should not have direct-to-consumer marketing ability. My bold prediction is that if we took commercials off the air, I would expect to see healthcare costs significantly lower.
As of November 30th, HHS Secretary nominee Robert F. Kennedy Jr. has announced he wants to pull the advertising off the air. Welcomed news, to be sure — let’s hope it passes all red tape.
Michel Albert Daher, Pharm. D, APh, is a community pharmacist who has owned and operated three pharmacies located in California and Oregon. He currently owns one in the Los Angeles Area, which specializes in Oncology and long-term care services. He graduated from the Oregon State University/Oregon Health and Sciences University College of Pharmacy in 2013. He completed a one-year residency in ambulatory care at the Old Town Clinic located in Portland, Oregon, where he operated a pharmacy-managed diabetes clinic, which encompassed additional treatment for hypertension, hyperlipidemia, vaccine administration, and heart failure. He is currently an adjunct faculty in the division of pharmacy practice at Marshall B Ketchum University located in Fullerton, Ca. He also holds the title of advanced practice pharmacist, which allows him to prescribe or hold medications and order and interpret lab results.
Advertisement